
Last Updated on August 12, 2024 by The SportsMD Editors Shoulder pain in an athlete is a very common malady. Pain in the shoulder can be debilitating for athletes of all ages and competition levels. One possible, but relatively uncommon cause of shoulder pain is called a deltoid strain.
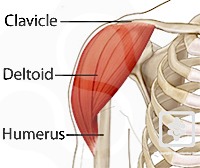
The deltoid muscle is a large muscle that encompasses the shoulder joint. The deltoid is divided into three different portions, or heads, the anterior (front), middle, and posterior (back) portions of the deltoid. The deltoid originates on the lateral aspect of the acromion and clavicle and then inserts on the lateral aspect of the humerus. Its major action is to abduct the arm (lift the arm out to the side of the body) as well as assist in forward elevation (lifting the arm out in front of the body). The deltoid is a very powerful muscle and is needed for all types of athletic endeavors.
Strains are injuries to muscles or muscle tendon units. Sprains are injuries to ligaments. Because the deltoid is a muscle, it can be strained, but not sprained.
There are many injuries in the shoulder that can mimic a deltoid strain. At times, these injuries can be difficult to distinguish one from the other. Some other things that can be injured include: the rotator cuff, glenoid labrum, biceps tendon, acromioclavicular joint (AC joint), shoulder dislocations, shoulder fractures, and soft tissue contusion. Many of these injuries can be treated conservatively, however some of these injuries require surgical intervention and need to be evaluated by a sports medicine physician to determine the extent of the injury.
Deltoid strains can be caused by numerous mechanisms. Most commonly they result from overuse of the muscle without adequate rest. This can lead to discomfort in the area of the deltoid muscle with associated swelling and loss of function. A forced eccentric contraction of the shoulder (lengthening of the muscle belly while contracting), can lead to strain of the deltoid muscle (ie: doing a “negative” while weight lifting). Less commonly, a direct traumatic blow to the shoulder can cause a deltoid strain.
Deltoid strains are diagnosed by looking at the mechanism of injury and the symptoms the patient is having at the time of injury. A physical examination is imperative. Patients with deltoid strains can have pain with palpation of the involved area of the deltoid muscle belly. In more severe cases, with actual tears of the muscle, a palpable defect may be felt. The shoulder is also assessed for swelling and skin changes. Range-of-motion and strength testing are done to help confirm the diagnosis of a deltoid strain and rule out other possible diagnoses.
Depending on the mechanism of injury, no imaging studies may be needed. If there is concern for fracture or dislocation, radiographs of the shoulder may be indicated. Additionally, if there is concern for rotator cuff injury or a torn labrum, then a MRI of the shoulder, on rare occasions, may be necessary.
Deltoid strains are graded based on the severity of the injury.
Grade 1 deltoid strains generally result in mild pain in the affected shoulder. Patients with grade 1 strains are able to use their shoulder and can lift their arms with minimal pain and are able to do push-ups without much difficulty. There will generally be minimal or no swelling.
Grade 2 deltoid strains are the next level of severity. This level of injury represents a partial tearing of the deltoid muscle. A patient with a grade II strain will have increased deltoid pain when lifting their arm. They may have difficulty doing push-ups or lifting their arm. There will generally be mild or moderate swelling.
Grade III strains are the most severe. A patient with a grade III strain typically has tearing of the deltoid muscle belly. The patients typically have severe pain and dysfunction in their arm. They are not able to use their arm for activities and will have moderate to severe swelling.
In general, deltoid strains are treated conservatively. For Grade I injuries, generally little treatment is needed. Initially, most patients can benefit from sports injury treatment using the P.R.I.C.E. principle – Protection, Rest, Icing, Compression, Elevation. Anti-inflammatory medications can be used to treat the pain symptomatically. Grade II injuries can be treated similarly. A brief period of physical therapy may be helpful to decrease pain and increase motion in the arm. Grade III injuries, the most severe, are treated with physical therapy and restricted activities. Consider shoulder bracing and shoulder ice packs for icing, protecting and resting the deltoid. Only on the very rare occasion would surgery be needed for a deltoid strain.
Mild sprains can be treated with P.R.I.C.E.
Protection. The purpose of protection is to avoid further injury to the area by protecting the injured structures. The type of protection used varies depending on the injured area but may include a sling, protective tape, or over-the-counter brace.
Rest. Avoiding activities that put a lot of stress on your arm and shoulder is crucial to promote healing and prevent complications. If you have to use your arm or shoulder, you can use a shoulder brace or sling, which is shown to improve pai. Besides, you may use an over-the-counter pain medication to reduce pain and inflammation.
Ice. Ice can help reduce pain and swelling, as it numbs the affected shoulder and decreases blood flow to the area. Apply ice—wrapped in a damp towel— to the shoulder for 15 minutes at a time, 3 to 4 times a day.
Compression. Wrap the shoulder with an elastic bandage or a compression wrap to reduce swelling and support your shoulder. Avoid compressing too tightly. Doing so can impair circulation to the area. If the compressed area feels numb or tingly, loosen the bandage.
Elevation. Keep the injured shoulder above the level of the heart as often as possible.
Depending on the severity of the strain, athletes healing time and return to sport can within in a day or two, or up to several weeks to months later. In order to safely return to athletic competition, the athlete must have regained all of their strength, as well as range of motion (ROM). After this has been regained, often sport specific exercises are initiated (such as a throwing program for the throwing athlete). Once the athlete is pain free, has full strength and ROM, and completed their sport specific exercises, if appropriate, then they may return to play without restriction. For minor, grade I, type injuries this can be done very quickly, whereas more severe grade III injuries may need several months of recovery. Return to play decisions should be determined under the guidance of a sports medicine professional and possibly an athletic trainer or physical therapist.
Everyday hundreds of athletes sustain suden trauma injuries – or an injury due to overuse. There are definately signs when you should seek an appointment with a sports medicine doctor to diagnose the injury and establish a treatment plan. These signs can include:

How severe is your injury? Do I need to see a doctor or can this be managed at home? What should be my treatment plan? SportsMD Virtual Urgent Care is available by phone or video anytime, anywhere 24/7/365. Learn more via SportsMD’s Virtual Urgent Care Service.